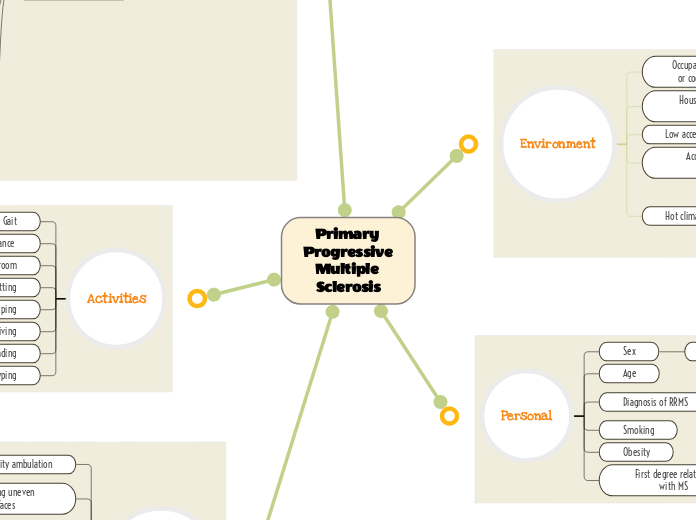
Primary Progressive Multiple Sclerosis
Environment
Occupation with physical or cognitive demands
House or apartment with stairs
Low access to vitamin D
Access to proper healthcare
Hot climates
Family lives in Florida, doesn't want to move up North, so just stays indoors during hot weather
Personal
Sex
Female
Age
Diagnosis of RRMS
Initially diagnosed with RRMS 2010 befrre PPMS
Smoking
Obesity
First degree relatives with MS
Body structures
T-cells destroy oligodendrocytes
Demyelination in the CNS
Slower action potentials
Fatigue
Weakness
Specific structures
Limbic system + frontal cortex
Trouble with processing, learning, and memory
Motor deficits
Fine motor
Gross motor
Olfaction problems
Optic nerve
Vision problems
Pons
Micturition/storage centers
Bowel, bladder issues
Cranial nerve nuclei 5-8
CN 7: facial nerve
Taste loss
Thalamic nuclei
Ventrolateral
Problems with active movements of the contralateral side
Spinal cord white matter
Fasciculus cuneatus/gracilis
DCML
Problems with proprioception and balance
Loss of sensation (fine touch, vibration)
Corticospinal tract
Foot drop
AFO
Hemiparesis
Activities
Gait
Balance
Using the restroom
Sitting
Sleeping
Driving
Reading
Typing
Participation
Community ambulation
Can't go to the store by herself
Ambulating uneven surfaces
Negotiating stairs
Unable to have stairs in the home
Recreational sports or activities
Activities of daily living
Cooking
Has special kitchen appliances that help with this
Cleaning
Struggles with hanging clothes
Dressing
Can only wear sports bras and shirts that can be pulled on
Showering
Shower has 2 grab bars
Deficits of PPMS
Fatigue
Neuroanatomy: myelin sheaths
Neurophysiology: saltatory conduction
Saltatory conduction makes neurons fire faster, without this myelination from the upper motor neurons, not as many action potentials will get through to the lower motor neurons, decreasing endurance of those structures.
Neuroplasticity: intensity matters, transference, specificity
The exercises should adequately challenge the patient, yet not overfatigue them
Including exercises and patient education in the pt's program that specifically addresses and helps improve fatigue
Working on endurance and managing fatigue symptoms will transfer over to improving her ability to attend longer social events
Objective measure: assessing RPE at the end of every exercise
To determine extent of fatigue and to set parameters of how intense exercises should be in regular POC and what the progression would look like; Follow up with questions about what type of fatigue the patient is feeling
Practice parameters
Distributed practice conditions should be utilized to ensure the patient's fatigue doesn't interfere with her treatment
Static balance
Neuroanatomy: DCML tract, corticospinal tract
Neurophysiology: with UMN lesions, the sensory input from the LMN cannot be processed, and the patient will have trouble with balance because the corticospinal tract is unable to receive proper information for how to engage muscles.
Neuroplasticity: repetition matters
Providing the pt a HEP that allows her to safely practice static balance in order to get the proper amount of repetitions in to make neuroplastic changes
Objective measure: dermatome testing
To figure out if the lack of balance is due to lesions to corticospinal tract or DCML
Loss of taste
Neuroanatomy: gustatory cortex, pons cranial nerve 7 nucleus
Neurophysiology: damage to the higher centers of gustation such as the cranial nerve 7 nuclei in the pons or the gustatory cortex will impede the patient's ability to sense taste.
Cognitive (Dual tasking)
Neuroanatomy: motor cortices, basal ganglia, limbic system, prefrontal cortex
Neurophysiology: Papez circuit located in the limbic system is involved with learning, the secondary motor areas help with external and internally guided movements, finally, the prefrontal cortex coordinates and controls these aspects of dual tasking via being in charge of working memory and attention.
Neuroplasticity: Salience matters, time matters, use it or lose it, interference
Make exercises functional to reinforce the Papez circuit and help with processing
It is important to note that she has been diagnosed with MS since 2010, so her brain will not make neuroplastic changes as easily as someone with a fresher brain injury
However this means that we need to start working on more neuroplastic changes ASAP because the sooner the better
Stimulating this area during PT will prevent further decline in cognitive processing
Since the patient has trouble with doing both cognitive and motor tasks at the same time, they compensate by stopping one task to complete the other. Slowly integrate dual tasking into treatment parameters.
Outcome measure: TUG and TUG cog (compare the two)
Measures cognitive dual tasking; patient starts from sit, stands up, and walks 3 meters and back while doing a cognitive task (ex: counting backwards from 100 by 5s), then sits down as quickly as possible
Practice parameters
At first we should break the dual tasking into parts, and then slowly integrate practicing both at the same time as a whole
Fine motor skills
Neuroanatomy: motor cortices, basal ganglia, thalamus, cerebellum
Neurophysiology: damage to the connections between the motor planning or coordination structures to the cortex, can cause discrepancies in fine motor skills. This input damage would be located to the area of the primary motor cortex that is in charge of moving the fingers.
Neuroplasticity: specificity, repetition matters, age matters
Incorporating a good HEP to get extra repetitions in for her fine motor exercises especially because this is one of her main goals
Including exercises that target the specific fine motor deficits that she struggles with
Taking her age into account, though it is possible to make neuroplastic changes, it may take a while compared to a younger patient
Professionally educate the patient about a realistic timeline and what it would take for how long it would take to achieve her goal to type with two hands
Outcome measure: nine-hole peg test
Measures hand dexterity; patient is timed and places the pegs in the holes as quickly as possible
Ambulation (dynamic balance)
Neuroanatomy: corticospinal tract, DCML tract
Neurophysiology: if there are problems processing information from the sensory tracts, the motor tracts will have problems integrating the proper ambulation pattern. In addition, with possible damage to the corticospinal tract, the patient experiences hemiparesis which further impedes gait skills.
Neuroplasticity: salience matters, transference,
Emphasizing that if ambulation improves, patient will be able to do more independent tasks by herself such as grocery shopping and socializing with friends.
When patient improves dynamic balances over firm surfaces, we can transfer her over to compliant surface ambulation to help her deficit of ambulating over uneven surfaces outside of the clinic.
Outcome measure: DGI
Determine what other parts of ambulatory activities the patient struggles with
Walking on level surface, changing gait speed, gait with horizontal and vertical head turns, gait with pivot turn, stepping over and around obstacles, walking up stairs
Practice parameters
The training for dynamic balance should be blocked at first to improve her foundations of gait then be transferred to random to mimic a variety of surfaces she'll encounter in her environment
Weakness
Neuroanatomy: Corticospinal tract
Foot drop
Left arm hemiparesis
Neurophysiology: the corticospinal tract travels through CNS white matter structures that may be damaged due to MS, in the spinal cord and brainstem
Efficacy of muscle contractions depend on this tract running through myelinated structures
Neuroplasticity: use it and improve it, use it or lose it, intensity matters, interference
Focusing on the weaker side of the body to improve its functions and recruitment
If you don't target the weak dorsiflexion and hemiparesis, it will atrophy and get worse
Making sure that the exercises that work the weaker muscles aren't too easy, and the patient feels challenged
If the patient has a steppage gait due to foot drop, it would interfere with learning a new gait pattern that involves active use of the weak dorsiflexors
Objective measure: MMT and ROM of anterior tibialis, extensor hallucis longus, extensor digitorum longus, as well as muscles of the shoulder, brachium and antebrachium
Guides POC to see extent of patient's weakness and to set intensity and modality of exercises given to pt
Loss of smell
Neuroanatomy: limbic system, olfactory cortex
Neurophysiology: damage to white matter in subcortical structures may affect smell due to the connections that the olfactory tract makes with the limbic system (amygdala, hypothalamus)
SMART Goals
Range of Motion
In 3 weeks, patient will improve dorsiflexion active range of motion by 5 degrees, to help prevent foot drop and thus fall risk during gait.
Fine motor
In 4 weeks, patient will score less than 33.3 seconds total on the 9-hole peg test to indicate improvement in hand dexterity and make strides towards typing with both hands