Genitourinary System Imaging
Functional Renal Imaging
Indications
-Evaluation of a renal transplant
-Evaluation of acute renal failure
-Measurement of relative renal function
Contraindications
-recent iodine contrast study
-pregancy
Patient Preparation
-patient history (abdominal surgery)
-Patient should hydrate well before exam
-void just before exam
Radiopharmaceutical
99mTc-MAG3 (Mertiatide)
Dose Amount
10-20 mCi
Facts
-Excreted by tubular secretion
-high first pass extraction fraction
-rapid plasma clearance
-Preferred over DTPA (Pentetate)
-Used for Effective Renal Plasma Flow (ERPF)
99mTc-DTPA (Pentetate)
Dose Amount
10-20 mCi
Facts
-Cleared by glomerular filtration
with minimal binding to the renal
parencyma
-Useful for Glomerular Filtration Rates (GFR)
-Useful for blood flow rates to each kindey
Technical Details
-Single or dual head gamma camera
-full field of view for adults
-LEAP (all purpose) collimator
-128x128 flow
-256x256 function
-Camera position posterior
-Camera anterior if previous kidney
transplant
Images
Flow
Renal Perfusion
-Dynamic acquisition
-30 frames x 2s/frame
-1 minute total time
Function
-Dynamic acquisition
-19 minutes of 20 s/frame
Post Void
-posterior static acquisition
for 2 minutes
Procedure
-Patient is supine
-one arm can be at patient's side and other
is placed on side table for easy flow injection
-bolus of rph inject via IV
-IV at antecubital preferred
-Sternal notch in top one third
of image
-Begin flow acquisition immediately
after injection
Normal results
-Renogram time activity curve
follows the expected projection
-Vascular Transit Phase
first 30-60 seconds
-Tubluar Concentration Phase
occurs 1-5 minutes, contains
peak curve
-Clearance/Excretion Phase
represents down slope of
curve
-Half-Time Excretion is the expected
half of the peak activity clearance
normally at 8-12 minutes
Diuretic Renal Scan
aka renal scan with lasix
Indications
-to distinguish between obstructive hydronephrotic
and non-obstructive collecting system dilation
-caused by vesicoureteral reflux, urinary tract infections,
congenital malformations, previous obstruction, or a
noncompliant bladder
-this test evaluates both renal function and urodynamics in
in a single test
Contraindications
-recent iodine contrast study
-pregancy
-dehydrated patients
Patient Preparation
-patient history (abdominal surgery)
-Patient should hydrate well before exam
-void just before exam
Radiopharmaceutical
99mTc-MAG3 (Mertiatide)
Dose Amount
10-20 mCi
Facts
-Excreted by tubular secretion
-high first pass extraction fraction
-rapid plasma clearance
-Preferred over DTPA (Pentetate)
-Used for Effective Renal Plasma Flow (ERPF)
99mTc-DTPA (Pentetate)
Dose Amount
10-20 mCi
Facts
-Cleared by glomerular filtration
with minimal binding to the renal
parencyma
-Useful for Glomerular Filtration Rates (GFR)
-Useful for blood flow rates to each kindey
-Not commonly used for diuretic renography
Pharmaceutical
-Furosemide (Lasix)
-40mg Dose IV inj
-Typically at 20 mins post rph inj
Technical Details
-Single or dual head gamma camera
-full field of view for adults
-LEAP (all purpose) collimator
-128x128 flow
-Camera position posterior
-Camera anterior if previous kidney
transplant
Images
Flow
Renal Perfusion
-Dynamic acquisition
-30 frames x 2s/frame
-1 minute total time
Function
-Dynamic acquisition
-20-40 minutes of 20 s/frame
Post Void
-posterior static acquisition
for 2 minutes
Procedure
-Patient is supine
-one arm can be at patient's side and other
is placed on side table for easy flow injection
-bolus of rph inject via IV
-IV at antecubital preferred
-Sternal notch in top one third
of image
-Begin flow acquisition immediately
after injection
-IV inject 40mg of furosemide (lasix) when
collecting systems are full, typically at
20 minutes post inject of rph
-Continue imaging for ~20 minutes
-Have patient void and take post void static
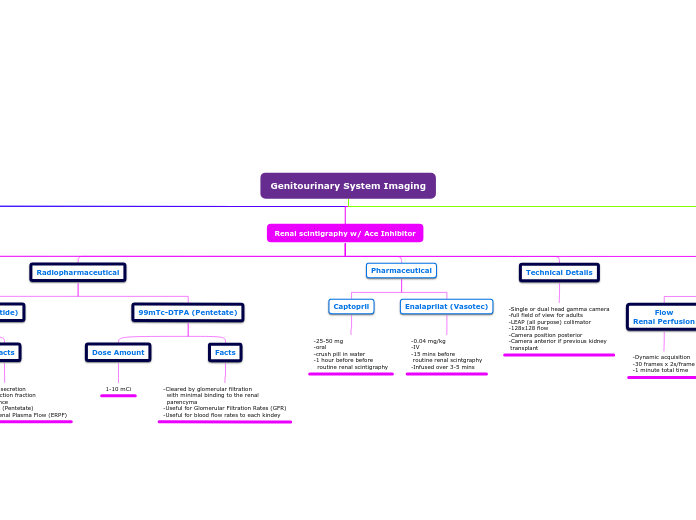
Renal scintigraphy w/ Ace Inhibitor
Indications
-Diagnosis or exclusion of Renal Vascular Hypertension (RVH)
-Differentiation of RVH from Renal Artery Stenosis (RAS)
Contraindications
-pregancy
Patient Preparation
-patient history (abdominal surgery)
-Only liquids for 4 hours before exam
-Patient should hydrate well before exam
-void just before exam
-halt captopril for 48hrs prior to exam
-halt enalaprilat or lisinopril 1 week before
Radiopharmaceutical
99mTc-MAG3 (Mertiatide)
Dose Amount
1-10 mCi
Facts
-Excreted by tubular secretion
-high first pass extraction fraction
-rapid plasma clearance
-Preferred over DTPA (Pentetate)
-Used for Effective Renal Plasma Flow (ERPF)
99mTc-DTPA (Pentetate)
Dose Amount
1-10 mCi
Facts
-Cleared by glomerular filtration
with minimal binding to the renal
parencyma
-Useful for Glomerular Filtration Rates (GFR)
-Useful for blood flow rates to each kindey
Pharmaceutical
Captopril
-25-50 mg
-oral
-crush pill in water
-1 hour before before
routine renal scintigraphy
Enalaprilat (Vasotec)
-0.04 mg/kg
-IV
-15 mins before
routine renal scintgraphy
-Infused over 3-5 mins
Technical Details
-Single or dual head gamma camera
-full field of view for adults
-LEAP (all purpose) collimator
-128x128 flow
-Camera position posterior
-Camera anterior if previous kidney
transplant
Images
Flow
Renal Perfusion
-Dynamic acquisition
-30 frames x 2s/frame
-1 minute total time
Function
-Dynamic acquisition
-1-2 mins/frame for 20-30 mins
Post Void
-posterior static acquisition
for 2 minutes
Procedure
-Administer Captopril or enalaprilat per required timing
prior to examination
-Record blood pressure every 15 mins after ACE
administration
-Perform routine renal scintigraphy with renography
-Obtain post void image
-At termination of imaging a final blood pressure reading
is taken
-Baseline renal scintigraphy needs to be performed before
or after Ace scan to compare results
Normal / Abnormal Results
-Patient test positive for RAS if two conditions are met:
1. Ace inhibitors study has a decrease of urine flow
2. Renal study without Ace shows improvement
compared to other study
Morphological Renal Scan
aka cortical imaging
Indications
-detects the amount of
functioning renal cortical tissue
-ex: detect small renal infarctions,
scaring, acute pyelonephritis (typically
caused by UTI)
-differentiate a prominent column of
Bertin from a true mass
Contraindications
-pregancy
-patient movement
Patient Preparation
-patient history (abdominal surgery)
-advise patient of exam and timing
-void just before exam
Radiopharmaceutical
99mTc-DMSA (Dimercaptosuccinic Acid
Dose Amount
5 mCi
Facts
-90% is bound to plasma protients
which prevents most glomerular filtration
-25-50% of the inject dose is in the kidney
with an increase over time
-DMSA is taken up in the renal cortex (proximal
convoluted tubal
-highest radiation dose of all renal due to much
longer retention
99mTc-GH (Gluceptate)
Dose Amount
10-15 mCi
Facts
-Secreted by glomerular filtration
and tubular secretion
-permits visuatization of renal blood
flow and imaging of renal cortex
-must be refrigerated
-50% renal clearance in 3 hours
Subtopic
Technical Details
- LFOV gamma camera
- parallel hole collimator for differential
calculation
-Pinhole collimator for cortical images
Images
Static Images
-Image Posterior
-Post/RAO/LAO/RPO/LPO
-500k total counts per image
-If pinhole is used 100k counts
or 5 mins
Procedure
-ID Patient, verify order, explain procedure
-Patient should void before starting
-Inject radiopharmaceutical via IV
-Image patient in supine position at
2-4 hours
Results
Normal
-Smooth renal contour
-uniform uptake of tracer concentration
Abnormal
-non uniform uptake/cold spots
-no uptake in column of Bertin is indicative of
tumor
Radionuclide Cystography
Indications
-Evaluation and detection of vesicoureteral reflux (VUR)
Contraindications
-pregancy
Patient Preparation
-cover imaging table with absorbent paper
-Patient should void prior to exam
-written consent for catheterization
-weigh new/clean diaper
-notate amount of saline from start to finish
Radiopharmaceutical Options
99mTc-Pertehnate
99mTc-DTPA
99mTc-Sulfur Colloid
Dose Amount
0.5-1mCi
Facts
-Radionuclide cystography is preferred to
iodinated contrast cystography
-tracer is injected into tubing connected to
bladder catheter
Technical Details
-Hang 500ml bag of normal saline
25 cm above table
-Image dynamic at 5 sec/frame for 60 seconds
-Fill bladder to max using formual:
(age+2)x30=volume of bladder in ml
Images
Filling Phase
-Dynamic at 5 seconds for 1 minute
Full Bladder Phase
-120 second immediate static of posterior
and right/left posterior obliques
Voiding Phase
-120 second immediate
post void static image
Procedure
-Have patient void before procedure
-inject tracer into tubing connected
to bladder catheter
-fill bladder until drip slows or voids
around catheter
-Monitor P-scope for signs of reflux
(record amount of saline used at the
time that reflux is seen)
-Take images of full bladder
-Record amount used to fill bladder
-Deflate folly balloon and take post void images
-measure urine (or weigh diaper)
-determine residual bladder volume (ml)
voided (ml) x Residual Counts/minutes
------------------------------------------
Max counts/min - Residual counts/minutes
Results
Normal
-No reflux visualized
-all or nearly all voided from bladder
Abnormal
-any activity in the upper urinary tracts at any of the phases