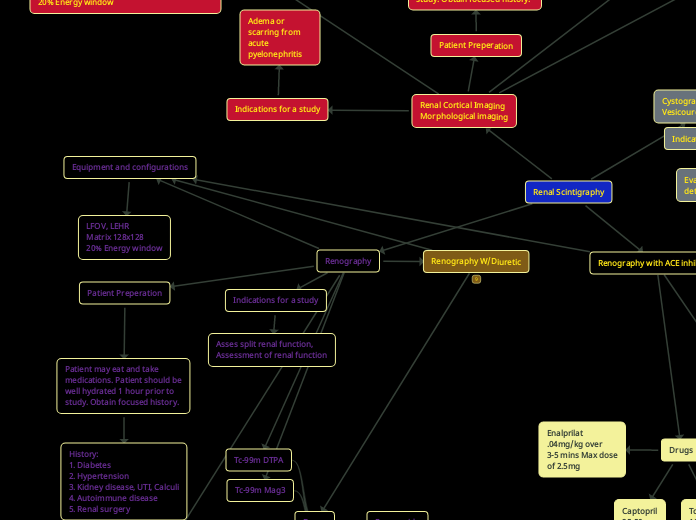
Renography
Equipment and configurations
LFOV, LEHR
Matrix 128x128
20% Energy window
Patient Preperation
Patient may eat and take
medications. Patient should be
well hydrated 1 hour prior to
study. Obtain focused history.
History:
1. Diabetes
2. Hypertension
3. Kidney disease, UTI, Calculi
4. Autoimmune disease
5. Renal surgery
Proceedure
Instruct patient to void immediately
prior to study. Position patient supine
with kidneys in FOV. Administer bolus
and begin imaging.
Acquisition:
Dynamic- 2-4 sec per frame for 60-120s
Static- 1-2 min per frame for 20-30 mins
View: Posterior
Renography W/Diuretic
Indications for a study
Asses split renal function,
Assessment of renal function
Drugs
Furosemide
Tc-99m DTPA
Tc-99m Mag3
Renal Scintigraphy
Renography with ACE inhibitor
Indications for a study
Differentiation of renal vascular
hypertension (RVH) from renal
artery stenosis. Diagnosis or exclusion
of RVH.
Proceedure
Baseline scan
Captopril should be taken orally 1 hour prior to procedure. Instruct patient to void immediately prior to study. Position patient supine with kidneys in FOV. Administer bolus and begin imaging.
Acquisition:
Dynamic- 2-4 sec per frame for 60-120s
Static- 1-2 min per frame for 20-30 mins
View: Posterior
ACE inhibition renogram
Patient should void prior to study.
Record patients blood pressure.
Renal Cortical Imaging
Morphological imaging
Indications for a study
Adema or scarring from acute
pyelonephritis
Drugs
TC-99m Gluceptate
10-15mCi
Children
200uCi/kg
Tc-99m DMSA
5 mCi
Pediatric dose
50uCi/kg
Patient Preperation
Patient may eat and take
medications. Patient should be
well hydrated 1 hour prior to
study. Obtain focused history.
History:
1. Diabetes
2. Hypertension
3. Kidney disease, UTI, Calculi
4. Autoimmune disease
5. Renal surgery
Proceedure
Instruct patient to void immediately
prior to study. Position patient supine
with kidneys and bladder in FOV. If using a
pinhole collimator, kidneys should fill 75% of FOV. Administer bolus and begin imaging. Patient should return after 2-4 hrs for additional static images. Obtain a pre-void and post-void bladder
image.
Acquisition:
Dynamic- 2-4 sec per frame for 60-120s
Static- 1-2 min per frame for 20-30 mins
SPECT (optional)
View: posterior, anterior for transplanted kidneys, RPO, LPO, RL, LL.
Cystography
Vesicoureteral reflux study
Indications for a study
Evaluation and detection of VUR
Patient preperation
Cover work area with absorbent paper.
Obtain consent for catheterization.
Patient may eat and take
medications. Patient should be
well hydrated 1 hour prior to
study. Obtain focused history.
History:
1. Diabetes
2. Hypertension
3. Kidney disease, UTI, Calculi
4. Autoimmune disease
5. Renal surgery
Equipment and configurations
LFOV, LEHR
Matrix 128x128
20% Energy window
Procedure
Insert catheter using aseptic techniques. Hang 500ml of normal saline 25cm
above table or chair. Position patient
supine or sitting upright. If patient can use
potty chair, place chair in front of camera with camera face posterior to patient. Inject RP into tubing connected to bladder catheter.Fill bladder to max capacity (age+2)x30=volume (ml)
Record the filling volume when reflux is first observed and at max filling. Obtain prevoid static images. Obtain multiple sequential voiding images by removing the catheter and having patient void. Obtain postvoid image.
Acquisition:
Dynamic- Filling/voiding (10-15s/frame)
Static- 120s
View: Posterior,
Additional views: RAO. LAO post infusion, postvoid.
Drugs
Tc-99m Sulfur colloid .5-1 mCi
Tc-99m DTPA .5-1mCi
Drugs
Captopril
25-50mg
Tc-99m Mag3
10 mCi
Enalprilat
.04mg/kg over
3-5 mins Max dose
of 2.5mg
Patient Preperation
Patient may eat and drink. Patient should be well hydrated 1 hour prior to
study. Diuretics should be discontinued for 3 days prior to study. ACE inhibitors should be discontinued 48 hrs prior for Captopril, and 1 week for Lisinopril or Enalprilat prior to study. Obtain focused history.
History:
1. Diabetes
2. Hypertension
3. Kidney disease, UTI, Calculi
4. Autoimmune disease
5. Renal surgery