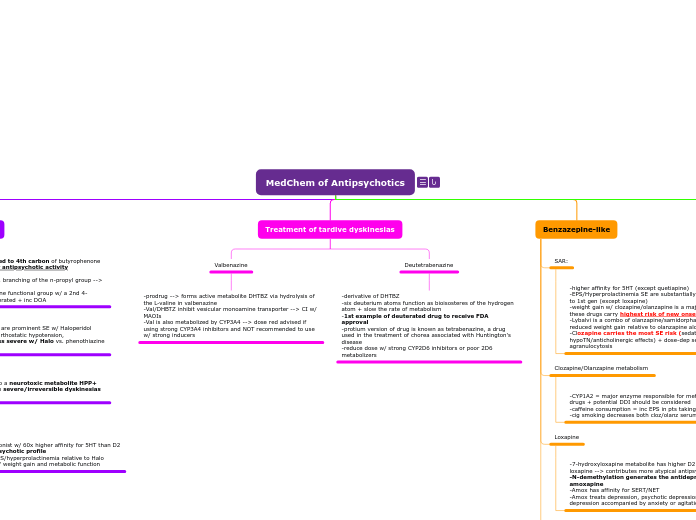
MedChem of Antipsychotics
Major Structural Classes of Antipsychotics
Phenothiazine-like
Drugs:
-Chlorpromazine
-Fluphenazine
-perphenazine
-thioridazine
-trifluoperazine
-thiothixene
Subtopic
Butyrophenone-like
Drugs:
-Haloperidol
-pimozide
-lumateperone
Benzazepine-like
Drugs:
-loxapine
-clozapine
-olanzapine
-quetiapine
-asenapine
Benzisoxazole-like
Drugs:
-risperidone
-paliperidone
-ziprasidone
-iloperi
-lurasi
-apiprazole
-brexipiprazole
-cariprazine
Phenothiazine-like
-drugs have equal or > affinity for D2 r vs. 5HT r --> sig EPS/hyperprolactinemia side effects
-sedation, orthostatic hypoTN, anticholinergic side effects are more severe with chlorpromazine/thioridazine
-piperazine-containing analogs have reduced affinity for H/M/a1A
Metabolism
-Oxidative N-dealkylation is a common meta pathway w/ many CNS drugs
-least sterically hindered carbon attached to the nitrogen atom will be hydroxylated by CYP450
-N-dealkylated metabolite is an active metabolite
-extensively meta by P450 in liver
-major diff for thiothixene metabolism relative to the phenothiazines is lack of ring-hydroxylated products
Chlorpromazine vs. thiothixene
Butyrophenone-like
-tertiary amine attached to 4th carbon of butyrophenone skeleton is essential for antipsychotic activity
-lengthening, shortening, branching of the n-propyl group --> dec antipsychotic act.
-replacement of the ketone functional group w/ a 2nd 4-fluorophenyl group is tolerated + inc DOA
SAR:
-EPS/hyperprolactinemia are prominent SE w/ Haloperidol
-Sedation, weight gain, orthostatic hypotension, anticholinergic SE are less severe w/ Halo vs. phenothiazine chlorpromazine
Metabolism:
-Halo --> CYP3A4
-HPTP metabolite leads to a neurotoxic metabolite HPP+ that may be implicated in severe/irreversible dyskinesias seen w/ halo therapy
Lumateperone
-potent 5-HT antagonist w/ 60x higher affinity for 5HT than D2 --> atypical antipsychotic profile
-reduced risk for EPS/hyperprolactinemia relative to Halo
-favorable safety w/ weight gain and metabolic function
Treatment of tardive dyskinesias
Valbenazine
-prodrug --> forms active metabolite DHTBZ via hydrolysis of the L-valine in valbenazine
-Val/DHBTZ inhibit vesicular monoamine transporter --> CI w/ MAOIs
-Val is also metabolized by CYP3A4 --> dose red advised if using strong CYP3A4 inhibitors and NOT recommended to use w/ strong inducers
Deutetrabenazine
-derivative of DHTBZ
-six deuterium atoms function as bioisosteres of the hydrogen atom + slow the rate of metabolism
-1st example of deuterated drug to receive FDA approval
-protium version of drug is known as tetrabenazine, a drug used in the treatment of chorea associated with Huntington's disease
-reduce dose w/ strong CYP2D6 inhibitors or poor 2D6 metabolizers
Benzazepine-like
SAR:
-higher affinity for 5HT (except quetiapine)
-EPS/Hyperprolactinemia SE are substantially reduced relative to 1st gen (except loxapine)
-weight gain w/ clozapine/olanzapine is a major challenge + these drugs carry highest risk of new onset diabetes
-Lybalvi is a combo of olanzapine/samidorphan that has reduced weight gain relative to olanzapine alone
-Clozapine carries the most SE risk (sedation/orthostatic hypoTN/anticholinergic effects) + dose-dep seizure risk and agranulocytosis
Clozapine/Olanzapine metabolism
-CYP1A2 = major enzyme responsible for metabolism of these drugs + potential DDI should be considered
-caffeine consumption = inc EPS in pts taking clozapine
-cig smoking decreases both cloz/olanz serum lvls
Loxapine
-7-hydroxyloxapine metabolite has higher D2 affinity than loxapine --> contributes more atypical antipsychotic profile
-N-demethylation generates the antidepressant amoxapine
-Amox has affinity for SERT/NET
-Amox treats depression, psychotic depression, and depression accompanied by anxiety or agitation
Quetiapine
-formation of the major quetiapine metabolite are catalyzed by CYP3A4
-norquetiapine is an active metabolite
-1st pass metabolism is extensive
Benzisoxazole-like
SAR
-all have higher affinity for 5HT (except lurasidone)
-EPS/hyperprolactinemia reduced
-lack anticholinergic activity + assoc. SE
-weight gain w/ ziprasidone and lurasidone is minimal
-risk for orthostatic hypoTN is greatest with risperidone/iloperidone
-Lura was designed w/ selectivity a1 adrenergic r in mind and has more than 100x preference for D2/5HT
Metabolism
-Resperidone is oxidized by CYP2D6 or CYP3A4 to paliperidone --> excreted unchanged through renal elimination
-CYP3A4/CYP2D6 mediated N-dealkylation is also observed
-Aldehyde oxidase (AO) is the major metabolic path for zipra
Aryl Piperazine antipsychotics
Drugs:
-Aripiprazole
-Brexipiprazole
-Cariprazine
SAR
-Aryl piperazine -> 5HT antagonists, D2 partial agonist --> risk of EPS/hyperprolactinemia LOW
-Brex --> higher affinity for D2/5HT
-Cariprazine is a D3 preferring compound (6x)
-these drugs lack anticholinergic activity + SE
-weight gain minimal with aripiprazole
Apiprazole
-potential for DDI w/ inhibitors/inducers
-modest elevation in plasma lvls in presence of CYP3A4 inhibitor/CYP2D6 inhibitor
-Plasma lvls dec in presence carbamazepine
Long-acting injectable antipsychotics
Drugs:
-fluphenazine
-haloperidol
-paliperidol
-Pro-drugs: hydroxyl containing antipsychotics can be esterified w/ saturated fatty acids, which upon IM injection depot in tissue and are slowly cleaved by esterase to release parent drug over time
-aripip lauroxil uses a methylene oxygen spacer to join the C12 fatty acid to the parent drug
Olanzapine Pamoate:
-insoluble salt that dissolves slowly after IM inj, thus its PK are an absorption-rate rather than elimination-rate controlled process
-long-acting inj versions of risperidone and aripip are available that employ formulation approaches for engineering extended release of drug