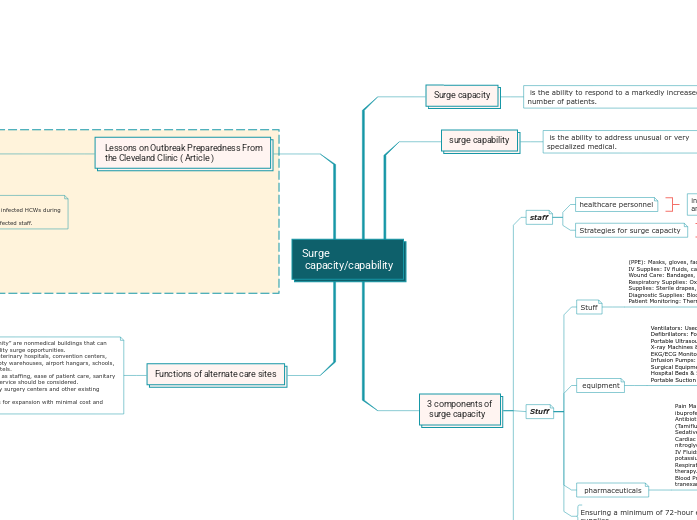
Surge
capacity/capability
Surge capacity
is the ability to respond to a markedly increased number of patients.
surge capability
is the ability to address unusual or very specialized medical.
3 components of
surge capacity
staff
healthcare personnel
Strategies for surge capacity
Stuff
Stuff
(PPE): Masks, gloves, face shields, gowns, shoe covers.
IV Supplies: IV fluids, catheters, syringes, needles.
Wound Care: Bandages, gauze, sutures, antiseptics.
Respiratory Supplies: Oxygen masks, nasal cannulas.
Supplies: Sterile drapes, scalpels, surgical sponges.
Diagnostic Supplies: Blood collection tubes, swabs.
Patient Monitoring: Thermometers, pulse oximeters, BP cuffs.
equipment
Ventilators: Used for respiratory support in critical care.
Defibrillators: For emergency cardiac resuscitation.
Portable Ultrasound Machines: For rapid diagnostics.
X-ray Machines & CT Scanners: For imaging and assessment.
EKG/ECG Monitors: For cardiac monitoring.
Infusion Pumps: For controlled IV medication delivery.
Surgical Equipment: Operating tables, anesthesia machines.
Hospital Beds & Stretchers: For patient transport and care.
Portable Suction Units: To clear airways.
pharmaceuticals
Pain Management: Morphine, fentanyl, acetaminophen, ibuprofen.
Antibiotics & Antivirals: Amoxicillin, ciprofloxacin, oseltamivir (Tamiflu).
Sedatives & Anesthetics: Midazolam, propofol, ketamine.
Cardiac & Emergency Medications: Epinephrine, atropine, nitroglycerin.
IV Fluids & Electrolytes: Normal saline, lactated Ringer’s, potassium chloride.
Respiratory Medications: Albuterol, corticosteroids, oxygen therapy.
Blood Products & Coagulation Agents: Plasma, packed RBCs, tranexamic acid.
Ensuring a minimum of 72-hour expendable supplies
Structure
Hospitals
such Primary healthcare facilities
Specialized treatment centers
Clinics/procedure facilities
such outpatient care centers, urgent care facilities
Mobile ( tents and trucks)
such mobile hospitals, Field medical stations, Emergency response units
Building of opportunity
such Hotels and vacant buildings
Lessons on Outbreak Preparedness From
the Cleveland Clinic ( Article )
Erica Orsini, in this article, discussed outbreak preparedness in hospitals, using lessons from the Cleveland Clinic's response to the COVID-19 pandemic. It outlines ten key principles for disaster planning.
Staff:
1. Poor PPE adherence – Many healthcare workers did not follow PPE protocols properly.
2. Misconception of correct PPE use – Caregivers believed they were using PPE correctly even when they were not.
3. Need for additional monitoring – A "buddy system" was required to ensure proper donning and doffing.
4. Training alone was not enough – Compliance improved but remained below ideal levels.
5. Need for Workforce Flexibility – Employees had to adapt to new roles, requiring cross-training and redeployment.
6. stressful for health care workers and their families from pandemic infection.
Stuff:
1. Resource Scarcity – Disasters create shortages due to poor planning, the disaster itself, or both.
2. PPE Shortages – Hospitals struggled to maintain adequate N95 mask supplies.
3. Higher PPE Usage – Initial PPE stockpiles were insufficient due to increased demand during outbreaks.
4. Supply Chain Disruptions – Fractured supply chains forced hospitals to conserve and reuse N95 masks
5. Healthcare Worker Shortages – Many hospital employees were unable to work.
6. Non-COVID-19-Related Absences – Some healthcare workers were unavailable for reasons other than infection.
Structure:
1. Workplace exposure risk – 50% of infected HCWs during H1N1 got the virus at work.
2. Alternative housing provided for infected staff.
Functions of alternate care sites
Facilities of opportunity” are nonmedical buildings that can
offer healthcare facility surge opportunities. Examples include veterinary hospitals, convention centers, exhibition halls, empty warehouses, airport hangars, schools, sports arenas, or hotels.
Considerations such as staffing, ease of patient care, sanitary
facilities, and food service should be considered. Facilities such as day surgery centers and other existing healthcare facilities
may provide options for expansion with minimal cost and
effort
including doctors, nurses, emergency responders, and support staff.
volunteer coordination, and temporary expansion of workforce capabilities.