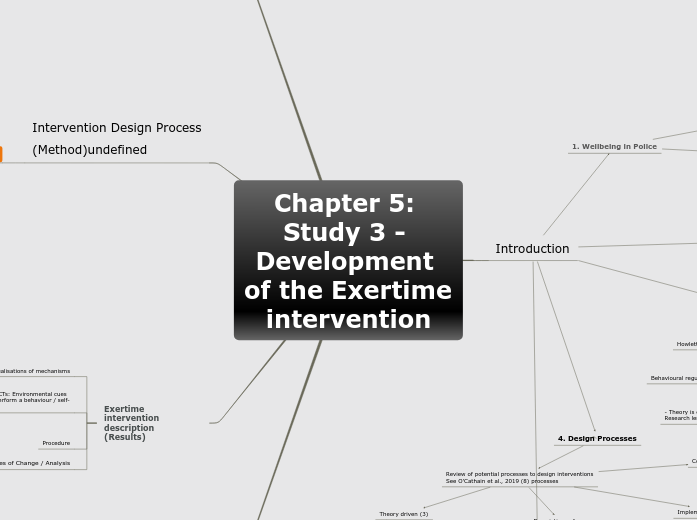
Chapter 5: Study 3 - Development of the Exertime intervention
Introduction
2. Worksite interventions to increase PA and decrease sitting
Shrestha et al., 2018 Cochrane review
->Sit-stand desks not effective
Stephenson et al., 2017 most freq:
Prompts and cues
Self-monitoring
Social support (unspecified)
Goal setting (beh)
-> Need improved reporting
Exertime = in police context
Pedersen et al., (2013)
Mainsbridge et al., (2014)
+ Blood pressure, calories
- No follow up
Mainsbridge et al., (2020)
+ Exertime Tasmanian Police
+ Mood (POMS-SF Vigor and Fatigue) N.S., Stress (PSQ-Op&Org) Org decreased.
+ 13 week post-test, 26 week washout
- PSQ-Op?
- Small sample
- Lack theoretical underpinning needed e.g. BCW
Cooley et al., (2014)
+ Qualitative follow-up
Quite a few qual studies:
Dewitt et al., 2019 (need org support)
But dont which department in police!
1. Wellbeing in Police
Impacts on health
Impacts on wellbeing
Non-operational staff e.g., control room overlooked
3. Theoretical underpinning
Howlett et al., 2020 COM-B and TPB predictive validity
Behavioural regulation, Social influences
- Theory is only one approach
Research lending from PA?
Habit strength
SDT (Kinnafick / Thorgersen-Ntoumani papers)
5. Aim and Objectives of the chapter
AIM: To develop and design an intervention to address low physical activity in two British police forces
OBJ 1: To use a co-design approach to develop a solution to prolonged sitting in the police control room context
OBJ 2: To use the Behaviour Change Wheel to design a theory-based intervention that reduces sitting time amongst police control room workers
OBJ 3: To plan for change (HNA Step 3)
O'Cathain et al., 2019:
Development = whole process of int developmet
Design = Point in process where developers decide content, format, delivery
4. Design Processes
Review of potential processes to design interventions
See O'Cathain et al., 2019 (8) processes
Descriptions of co-design principles office setting
Target population-centred (2) Participatory
SMArT Work
Munir et al., 2015 Protocol
+ Systematic BCW
+ Support through researcher
How as important as what!
e.g., Hardcastle et al., 2017
Edwardson et al., 2018 RCT
+ Effective long-term
- Support measure broad
Double Diamond (1 - Partnership)
Efficiency based (5) Stand Up Victoria
Neuhaus et al., 2014
+ Iterative development
+ Multi-level, multi-component
-> Bryne et al., 2020 need causal pathways
MoA (Carey et al., 2018), need to isolate BCT effects (Hagger et al., 2020)
Dunstan et al., 2013 Protocol
- Measures
Hadgraft et al., 2017 RCT
-> Need to understand interpersonal infl
-> Bryne et al., 2020 need context to advance field
Miller et al., 2019 review
Hadgraft et al., 2016 Qual
Theory driven (3)
BCW
+ Widely used, BCTs comparable
- Need to make MoA & causal pathways clear
- Final decision with researcher
Koykka et al., 2019
(Action planning - habits)
+ Multiple theories - BCW, TPB, IM
+ Paid attention to context (teachers)
Other frameworks or theroeis that could have been used
Intervention mapping
(see concepts Golden Hours v0)
MRC
Implementation based (4) RE-AIM
MacDoanld et al., 2018 systematic review.
Reach and efficacy most reported.
Implementation reporting mixed.
Low adoption and maintenance reported
Combined approach (8)
Needs to be formal?
Discussion
Reflections BCW / DD / My process
BCW could benefit from some iterations - whole 2nd DD
Covid-19 section
Things the intervention couldnt do, but would have
Lost some BCTs (1.9, 4.1, 8.1)
No face to face suppot or training session
Objective measures - blood pressure, activPAL...
Personal reflection
Context completely changed (social norms as influential now?)
Chapter 6??
Changing personnel (6 month role rotation?)
Intervention Design Process
(Method)undefined
The Behaviour Change Wheel
STEP 1: COM-B: Understand the behaviour
Defining the problem
Select target behaviour
Specify target behaviour by discussing / justifying focus with supervisory team
Identify what needs to be changed
TDF optional step
STEP 2: Identify intervention options
Identify what you want intervention to do: Modelling and Environmental restructuring. APEASE criteria
Policy categories
STEP 3: Identify content (Behaviour change techniques) and implementation options
Present options to steering group, with consideration of criteria
Discuss with supervisors
Identify mode of delivery
Double Diamond 1
BCW = DD Phase 1 DISCOVER and DEFINE [STAGE 1]
DD Phase 2 DISCOVER and DEFINE [STAGE 2]
Feasibility of options through shift shadowing
I assessed feasbility through my own judgement? No progression criteria were applied, no one has checked the software actually fits with funcitonality of critical computer systems...
Final intervention descrption
Double Diamond 2
DD DEVELOP [STAGE 3]
Presented options for software to the steering group
DD Phase 3 DELIVER, DEVELOP, DELIVER [STAGE 4]
DELIVER sessions to supervisors
DEVELOP relationships with those assisting and DELIVER STAGE 4 = start with identifying SPOCs?
Exertime intervention description
(Results)
Conceptualisations of mechanisms
Describe, operationalise and justify BCTs: Environmental cues and promps / instruction on how to perform a behaviour / self-monitoring / social support
Raising awareness - sitting invisible (Gardner et al., 2019)
Descriptive norms (Kim et al., 2017 PA; Preibe & Spink, 2011 SB)
Procedure
Measures of Change / Analysis
Protocol paper:
AIM: To describe the protocol for the Exertime RCT
OBJ 1: To use the TIDieR checklist to report the Exertime intervention and ensure high quality description
OBJ 2: To understand the value of behavioural regulation and social influence mechanisms in the Exertime intervention
OBJ 3: To outline the use of the RE-AIM framework to evaluate the Exertime intervention
INTRO
Combined approach of theory-based co-design, and implementation based processes
Using RE-AIM as process evaluation (not just efficacy important), and in line with other recommendations – see MacDonald et al., 2018. So can be compared and add to literature base.
Discussion prev lit all focused on decreased sitting
METHOD
Designed using BCW and co-design desribed elsewhere
Procedure
TABLE mapping BCTs and operationalisation
Analysis
REACH
EFFICACY
2 x 2 x 2 Design so that know which mechanisms were effective
ADOPTION
IMPLEMENTATION
Treatment Fidelity Framework
MAINTENANCE