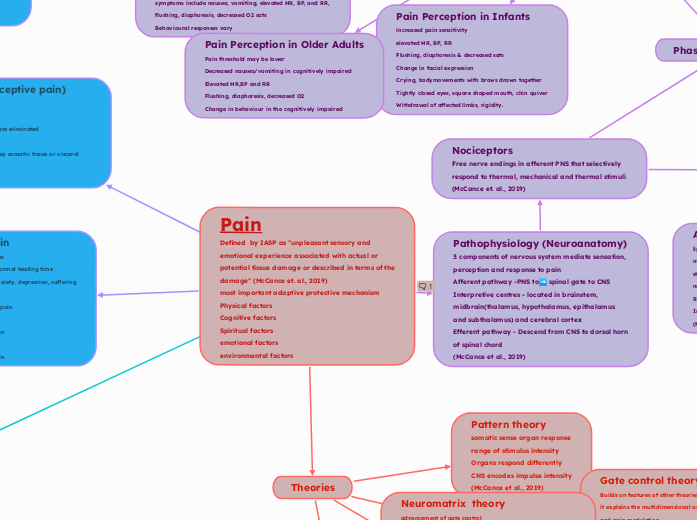
Pain
Defined by IASP as "unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of the damage" (McCance et. al., 2019)
most important adaptive protective mechanism
Physical factors
Cognitive factors
Spiritual factors
emotional factors
environmental factors
Theories
Specificity theory
intensity d/t amt of tissue injury
Pricking finger vs cutting hand
Applies to acute pain
(McCance et al., 2019)
Pattern theory
somatic sense organ response
range of stimulus intensity
Organs respond differently
CNS encodes impulse intensity
(McCance et al., 2019)
Gate control theory
Builds on features of other theories of pain
it explains the multidimensional aspects of pain perception and pain modulation
Pain transmission is regulated by impulses to the spinal cord, where substantia gelatinosa cells act as a gate.
Spinal gate regulate pain transmission to higher centres in CNS
Large myelinated a-delta + small unmyelinated C fibres respond to painful stimuli
Fibres terminate in interneurons of substantial gelatinosa and open spinal gate to transmit perception of pain
Nociceptive stimulation (touch sensor)
Spinal gate closure from nonnociceptive A-beta fiber stimulation reduces pain perception.
(McCance et al., 2019)
Neuromatrix theory
advancement of gate control
brain produces inputs patterns of impulses from various inputs
genetic
sensory-discrimative
affective
motivational
evaluative cognitive
Patterns may originate from brain with no external input
Pain experiences involve extensive network of brain regions
Showcases the plasticity of brain
Provides a holistic consideration of pain
Pain can be felt in the absence of input i.e phantom limb pain
(McCance et al., 2019)
Pathophysiology (Neuroanatomy)
3 components of nervous system mediate sensation, perception and response to pain
Afferent pathway -PNS to➡️ spinal gate to CNS
Interpretive centres - located in brainstem, midbrain(thalamus, hypothalamus, epithalamus and subthalamus) and cerebral cortex
Efferent pathway - Descend from CNS to dorsal horn of spinal chord
(McCance et al., 2019)
Nociceptors
Free nerve endings in afferent PNS that selectively respond to thermal, mechanical and thermal stimuli (McCance et. al., 2019)
Types
A-delta fibres
lightly myelinated fibres
medium sized fibres
stimulated by mechanonociceptors and/or mechanothermal nociceptors
Rapidly transmit "fast" pain sensations
Initiates reflex withdrawal before pain sensation is perceived
(McCance et al., 2019)
Unmyelinated
C-fibres
Polymodal
Stimulated by mechanical, thermal and chemical nociceptors
Slowly transmit dull, aching or burning sensations
Sensations are poorly localized and longer lasting
(McCance et al., 2019)
A- beta fibres
Large myelinated
Transmit touch and vibration sensations
Donot normally transmit pain
Play a role in pain modulation
(McCance et al., 2019)
Phases of Nociception
Transduction phase
Stimulation of nerves in periphery
Begins with tissue damage due :
exposure to Inflammatory chemicals stimuli (bradykinin, histamine, leukotreines, prostaglandins, interleukins (IL-1, IL-6, IL-7, IL-17)
mechanical or thermal stimuli
Nociceptors activated
(McCance et al., 2019)
Transmission phase
conduction of impulse along A-delta and C fibres into dorsal horn of spinal cord (primary order neurons)
Synapses formed with excitatory or inhibitory interneurons (2nd order neurons)
Impulse synapse with projection neurons (3rd order neurons)
Impulse crosses midline of spinal cord to brain through 2 spinothalamic tracts.
anterior spinothalamic carries fast impulse (acute sharp pain)
lateral spinothalamic carries slow impulse (dull/chronic pain)
Impulse project to somatosensory cortex for interpretation/intensity - to other areas for response
(McCance et al., 2019)
Perception phase
conscious awareness of pain
Takes place primarily in reticular, limbic systems and cerebral cortex.
Made of 3 systems' interactions - Sensory-discriminative system., affective-motivational system and cognitive-evaluative system
Pain perception changes with age
(McCance et al., 2019)
Sensory-discriminative system
mediated by somatosensory cortex
Identifies presence, character location and intensity of pain
(McCance et al., 2019)
affective-motivational system
behaviours and response to pain
mediated through reticular formation, limbic
Projects to prefrontal lobe
(McCance et al., 2019)
Cognitive-evaluative
system
Learned behaviour of pain experience
can modulate perception of pain
mediated through cerebral cortex
Pain threshold and tolerance are subjective and influence individual's perception of pain
Gender, genetics, culture, role expectations, role socialization, age, physical and mental health influences occur
(McCance et al., 2019)
Pain Perception in Children
Pain threshold lower than in infants
symptoms include nausea, vomiting, elevated HR, BP, and RR, flushing, diaphoresis, decreased O2 sats
Behavioural responses vary
Pain Perception in Infants
increased pain sensitivity
elevated HR, BP, RR
Flushing, diaphoresis & decreased sats
Change in facial expression
Crying, bodymovements with brows drawn together
Tightly closed eyes, square shaped mouth, chin quiver
Withdrawal of affected limbs, rigidity.
Pain Perception in Older Adults
Pain threshold may be lower
Decreased nausea/vomiting in cognitively impaired
Elevated HR,BP and RR
Flushing, diaphoresis, decreased O2
Change in behaviour in the cognitively impaired
modulation phase
Different mechanisms increase/decrease pain signal transmission
Can occur before, during or after pain perception (McCance et. al., 2019)
Descending Inhibitory Pathway
neurotransmitters inhibit/facilitate pain
Afferent stimulation of PAG+raphe nucleus = efferent pathway stimulation = afferent pain signal inhibited @ dorsal horn
RVM stimulate efferent pathways = facilitation/inhibition of pain @ dorsal horn
Inhibitory pathways activate opioid receptors = inhibitory neurotransmitters released
(McCance et al., 2019)
Segmental inhibition pathway
A-beta, A-delta and C fibre impulses arrive at same time at spinal level
Decrease in pain transmission occurs
example rubbing injured area for pain releif
(McCance et al., 2019)
Conditioned pain modulation pathway
Pain releif when 2 stimuli occur at same time from different sites
spinal-medullary-spinal pathway
basis of non pharmacological therapy i.e (acupuncture, cold/heat therapy
(McCance et al., 2019)
Placebo/Nocebo effect pathway
Cognitive expectations (Placebo = positive expectation, nacebo = negative expectations
(McCance et al., 2019)
Neurotransmitters
Diverse Group of chemical messengers (Chu et al., 2024)
Inflammation - mediator of excitatory neurotransmitters
Bradykinin, Leukotrienes, Prostaglandins, TNF-Alpha, Nitric Oxide, Substance -P, ATP
Cause release of substance P, CGRP, ATP.
Excitatory neuroTransmitters in brain and spinal cord
Reduce activation thresholds = increased nociceptor responsiveness
Glutamate, Aspartate, Substance P, Calcitonin
Inhibitory neurotransmitters
GABA, Glycine, norepinephrine, serotonin
Endogenous Opioids
inhibit pain impulse in brain, spinal cord and periphery
(McCance et al., 2019)
Enkephalins
most prevalent of natural opioids found in
Hypothalamus
PAG matter
medulla
dorsal horn
endormorphins
Bind with receptors in brain, brainstem and GI tract
Analgesic and antiinflammatory effects
(McCance et al., 2019)
dynorphins
most potent endogenous opiod
bind with K receptors = blocked pain signal in brain
Involved in mood disorder and drug addiction
(McCance et al., 2019)
endorphins
They are endogenous morphins
Produced in brain
beta-endorphin binding in hypothalamus +pituitary gland =exhiliaration and natural pain releif
(McCance et al., 2019)
Acute Pain (nociceptive pain)
Lasts seconds to days
Sudden
relived when pain mediators are eliminated
Anxiety is common
Arises from cutaneous and deep somatic tissue or visceral organs
Somatic Pain
occurs from muscle, bone, joints and skin
Sharp and well localized (A-delta fibres transmission)
Dull aching (C fiber transmission)
(McCance et al., 2019)
Visceral pain
Transmitted by C fibres
Pain in internal organs and lining of body cavities
Transmitted by sympathetic affarents
Poorly localized - less nociceptors in visceral structures
Associated with nausea/vomiting, hypotension, restlessness, shock
Often radiates
(McCance et al., 2019)
Referred pain
Felt in area away from point of origin
Impulses convey from several visceral neurons to one ascending neuron
Becomes hard for brain to distinguish
More receptors on skin promote pain experience at referred site.
(McCance et al., 2019)